Contents
August 12
and 14, 2008
General
Appearance, Vital Signs, and Mental Status Exam
|
____ Casual Observations of General Appearance ____ General
appearance: manner of dress, grooming,
alertness, clarity of thought and articulation ____ Body
habitus: physique, posture, proportions, asymmetry, strength, agility,
fluidity of motion, balance, tremor ____ Speech:
inflection, tone, volume, word choice ____ Psychological:
mood, eye contact, facial expression, body position, signs of distress,
attitude toward interview/examination |
Vocabulary ·
central obesity ·
cachexia ·
hypomania ·
psychomotor
slowing ·
tangentiality ·
bradykinesia ·
Korotkoff
sounds ·
systolic and
diastolic pressure ·
pulse pressure ·
white coat
hypertension ·
delirium ·
dementia |
|
Vital
Signs ____ Measure the blood pressure Locate the brachial artery pulse. Place cuff snugly with the marker above the artery Inflate
the cuff quickly to 30 mmHg above the systolic pressure as noted by the disappearance
of Korotkoff sounds or by the disappearance of the brachial pulse. Deflate
the bladder 3 mmHg per second Record
the pressure at which the pulse is first heard (or brachial pulse is first
felt) Record
the disappearance as the diastolic pressure (or in children, the point of
muffling) ____ Count respiratory rate for 30 seconds. ____ Palpate radial pulse and count for 15 seconds. |
Key knowledge Standards
for blood pressure measurement: ·
BP should be
taken after the patient has been sitting quietly with the back supported for
five minutes in a warm, quite setting. ·
The arm is
supported at the level of the heart. ·
No caffeine or
smoking during the prior hour ·
No
decongestants or eye drops for pupillary dilatation ·
The length of
the bladder should be 80 percent of the circumference of the upper arm. ·
While taking
the BP, Korotkoff sounds sometimes fade away just below the systolic pressure
and then reappear at a lower pressure (an auscultatory gap). This is why it is important to inflate the
cuff at least 30 mmHg above the disappearance of the pulse. ·
Take at least
two readings, separated by as much time as possible ·
For the
diagnosis of hypertension, two or more readings at each of two or more office
visits. ·
Check blood
pressure in both arms; if pressures differ, use the higher arm ·
If the arm
pressure is elevated, take the pressure in one leg, particularly in patients
under age 30 |
|
Mental
Status Exam - The Mini-COG (for appropriate patients) ____ Instruct the patient to listen carefully to and
remember 3 unrelated words. Have them
repeat the words back to you. ____ Perform the clock-drawing
test (CDT):
Instruct the patient to draw the face of a clock. Use either a blank sheet of paper or a
sheet with a circle already drawn on the page. After
the patient puts the numbers on the clock face, ask him / her to draw the
hands of the clock to read a specific time, such as “Ten ‘till two.” These
instructions can be repeated, but no additional instructions should be given.
Give the patient as much time as needed to complete the task. The CDT serves
as the recall distractor. ____ After the CDT, ask the patient to repeat the 3
previously presented words. |
Key Knowledge The Mini-Cog assessment instrument combines an uncued
3-item recall test with a clock-drawing test (CDT). The Mini-Cog can be
administered in about 3 minutes, requires no special equipment, and is
relatively uninfluenced by level of education or language variations. Scoring
for the Mini Cog Give 1
point for each recalled word after the CDT distractor. Score 1-3. -
A
score of 0 indicates positive screen for dementia. -
A
score of 1 or 2 with an abnormal CDT indicates positive screen for dementia. -
A
score of 1 or 2 with a normal CDT indicates negative screen for dementia. -
A
score of 3 indicates negative screen for dementia. The CDT is considered normal if all numbers are present
in the correct sequence and position, and the hands readably display the
requested time. |
|
Documentation Skills - On paper, document your findings from the above
exam. ____ Write a sentence that creates a snapshot
description of the general appearance and characteristics of your patient. ____ Record the patient's vital signs including the
units of measurement. ____ Record the results of the Mini-COG |
|
|
|
|
August 19
and 21, 2008
|
Skin ____ Inspect face, hair,
scalp, and palpate skull. |
Vocabulary ·
Pinna ·
Tympanic
membrane ·
Ossicles Key Knowledge Normally,
air conduction is better than bone conduction. With conductive hearing loss, bone
conduction is better. With
sensorineural deafness, both air and
bone conduction are impaired to the same degree. In
the Weber test, normally sound is heard in the center. With conductive hearing loss, the sound is
heard best on the affected side. With
sensorineural hearing loss, the sound is heard best on the other (unaffected)
side. Vocabulary ·
Conjunctiva ·
Anterior and
posterior chambers ·
Fundus ·
Optic disk ·
Fovea ·
Cataract ·
Hemianopsia Key knowledge In older patients,
cataracts can interfere with the visualization of the fundus. Therefore a quick inspection of the
anterior chamber and lens should precede fundoscopy. Cataracts will appear as black opacities in
the red reflex. |
|
Ears ____ Inspection, gentle tug
on pinna ____ Screen for hearing loss (occlude one ear canal and
softly say a word into the other) (CN VIII).
____ Rinne test to compare air and bone conduction. ____ Weber test to assess for lateralization. ____ Otoscopic examination of the auditory canals |
|
|
Eyes ____ Inspect the eyelids, lacrimal duct, conjunctiva
and cornea of each eye. ____ Measure visual acuity using a pocket Snellen
card (CN II). ____ Observe direct and consensual pupillary
responses (CN III). ____Test visual fields in each eye by confrontation.
Cover one eye with one hand. Have the patient look at your nose. Stretch
your arms out, with your fingers in a V-for-Victory sign. Move your hands in
to the periphery of your own vision. Wiggle
one set of fingers, and ask the patient if he/she sees anything move. Change
position of your hands to check both sides, as well as inferiorly and
superiorly. ____ Perform an ophthalmoscopic exam Adjust
panoptic settings. Use the small
circle for illumination. Focus on your
hand held 15-20 inches away from the panoptic. Place patient in stable, comfortable position. Dim
room lights. Have patient fix gaze on
a distant point. Start
2-3 feet from the patient looking through the iris at the red reflex,
checking for opacities. Move
15 degrees temporal to patient’s line of sight and advance, keeping red
reflex in view, until the rubber cone is gently applied to the patient’s
brow. You should see the retinal
vessels. Follow
the vessels centrally to inspect the optic disk, then outward into each of
the four quadrants. |
|
|
Nose / nasal passages ____ Inspection of the external nose ____ Palpation of the frontal and maxillary sinuses ____ Check for patency of both nasal passages ____ Examine nasal passages using a nasal
illuminator ____ Transilluminate the maxillary sinuses |
Vocabulary: ·
Nasal septum ·
Turbinates
(nasal concha) ·
Paranasal
sinuses ·
Mucosa |
|
Mouth ____ Inspect lips ____ Using a tongue depressor, inspect teeth, gums,
tongue, palate. ____ Inspect floor of mouth and base of tongue. ____ Observe elevation of the palate by asking
patient to say “ah” (CN IX) ____ Inspect posterior pharynx. ____ Perform palpation of the base of the mouth. |
Vocabulary: ·
Buccal mucosa ·
Anterior and
posterior pillars ·
Uvula ·
Parotid duct
(Stensen’s duct) |
|
Neck ____ Inspection of the neck. ____ Palpate lymph nodes: occipital, posterior
auricular, posterior cervical, anterior cervical, preauricular,
submandibular, submaxillary, submental ____ Supraclavicular nodes (while patient takes a
deep breath) ____ Palpate thyroid gland from behind or side. Note motion while patient is swallowing a
sip of water. ____ Palpate carotid pulses. ____ Auscultate carotids. Instruct patient to hold his/her breath as
you listen (hold your breath at the same time so you will remember to tell
patient to “stop breathing”........ “Breathe”). |
Vocabulary ·
Adenopathy ·
Goiter ·
Carotid
arteries ·
External
jugular veins |
|
Documentation Skills - On paper, document your findings from the above
exam. ____ Skin ____ Ears ____ Eyes ____ Nose ____ Mouth ____ Neck |
|
|
Reference: Swartz MH, Textbook of Physical Diagnosis, Saunders
(2006), pages 302-305. |
|
August 26
and 28, 2008
|
Skin ____ Examine the skin of the back and shoulders for
lesions, sum damage, bruising. Back ____ Inspect posture and spinal curvatures from the
patient’s side and from the back. ____ Test flexion, extension, and rotation of neck. ____ Palpate cervical vertebrae, and assess for
tenderness/spasm in the cervical musculature. ____ Gently perform fist percussion thoracic and
lumbar vertebrae, assessing for tenderness.
____ Palpate sacroiliac joints bilaterally for
tenderness. ____ Test flexion by having patient bend at waist to
touch toes. ____ While bending forward, check for scoliosis. ____ Have patient bend to each side from the waist. ____ Test spinal extension by having the patient
bend backwards. |
Vocabulary ·
Cervical ·
Thoracic ·
Lumbar ·
Sacral ·
Kyphosis ·
Lordosis ·
Scoliosis Key knowledge In older adults, problems
of the spine are among the most common disabilities. |
|
Thorax ____ Observe and describe the general configuration
of the chest. ____ With hands on the back, check for symmetry of
thoracic excursion. ____ Palpate above the suprasternal notch for
tracheal deviation. |
Vocabulary ·
Sternum ·
Manubrium ·
Costochondral
junctions ·
Costal margins ·
Tracheal,
bronchial, bronchovesicular, and vesicular breath sounds ·
Crackles,
wheezes, rhonchi ·
accessory
muscles respiration Key knowledge The surface landmarks of
the chest help to locate the underlying organs. Important landmarks include the angle of
Louis, the second intercostal space, and the numbered interspaces below that. Key references are the midclavicular line,
the anterior axillary line, and the posterior axillary lines. Key knowledge The breath sounds are
generated by airflow in the larger, central airways, and conducted through
the lung tissue to the chest wall. |
|
Lungs ____ Describe the patient’s respiratory status. ____ Ask patient to cross arms to move scapulae and
expose lung fields. ____ Percuss lung fields posteriorly, laterally, and
anteriorly. ____ Instruct patient to breathe through open mouth.
____ Auscultate posterior, lateral and anterior lung
fields and supraclavicular fossae, moving from side to side to check for
symmetry. ____ Using the heel of the hand, check tactile
fremitus, holding the hand against the posterior lung base while asking the
patient to say, “One, two!” Documentation skills - on paper, document your findings from the above
exam. ____ Skin ____ Spine ____ Thorax ____
Lungs |
September 2
and 4, 2008
|
Note: Measurement of vital signs has been covered in
Session 1. Auscultation of the carotid
arteries has been covered in Session 2.
The aorta and femoral arteries will be examined in Session 5, and the
pulses of the arms and legs in Session 6.
Although separated in this course, these parts of the cardiovascular
exam are often performed together. With the
patient sitting, leaning forward, listen with the diaphragm at the left
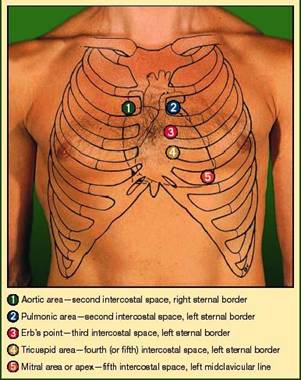
sternal border. ____ Listening at Erb’s point (l the diagram below) focus on systole (for a
mid-systolic click or late systolic murmur – of mitral valve prolapse). ____ Then, a little bit lower (m on the diagram below) and with firm pressure focus
on diastole (for a high-pitched decrescendo diastolic murmur – of aortic
insufficiency). ____ Also, listen for a friction rub. Now with
the patient supine, head elevated 30°, observe and examine the skin ____ Skin.
Examine the skin of the anterior chest for scars, nevi, rash, and
spider angiomas. Observe
and examine the neck ____ Observe for jugular venous distension, and
estimate the jugular venous pressure. You may need to move patient
progressively more upright. ____ Perform the abdomino-jugular test
(hepato-jugular reflux). ____ Palpate the carotid arteries. ____ Note the pulse contour. ____ Observe the rhythm of the pulse. Observe
and examine the chest ____ Observe precordium for asymmetry, deformities,
heaves, or apical motion. ____ Palpate for lifts or heaves with the heel of the
hand pressing firmly over the lower left sternal border. ____ Palpate for the presence, location, and
size of the apical impulse. ____ Percuss in the left 5th intercostal
space for the transition from dullness to resonance (men only). Listen with
the diaphragm to the aortic area j ____ Focus on systole, listening for a systolic
murmur. If present, assess its shape,
radiation, pitch and intensity. Listen
with the diaphragm to the pulmonic area k
____ Focus on S1 (splitting?) and any
sounds around it (ejection click?). ____ Then focus on S2 (physiologic
splitting?). ____ Then systole for murmurs. ____ Then diastole for murmurs. Listen
with the diaphragm to the tricuspid area m ____ Focus on systole for murmurs and midsystolic
clicks. ____ Focus on diastole listening for an opening snap
following S2 (from ASD or Ebstein’s anomaly). Switch to
the bell at the tricuspid area m ____ Use light pressure. Focus on diastole for S3 or S4
gallops or a low pitched rumbling murmur. Turn the
patient on the left side (lateral decubitus) ____ Palpate for the apical impulse and note whether it
is sustained, single or double (or even triple) in contour. Listen
with the diaphragm to the mitral area n ____ Focus on S1, ____ Then focus on S2, ____ Then systole for murmurs, ____ Then diastole for an opening snap following S2. Switch to
the bell at the mitral area n ____ Focus on diastole listing for S3
or S4 gallops, and for a low pitched rumbling decrescendo murmur. Documentation
skills - on paper, document your findings from the above exam. ____ Jugular veins /
abdomino-jugular test ____ Carotid arteries ____ Precordial palpation ____ Cardiac auscultation |
Vocabulary ·
Aortic,
pulmonic, mitral, and tricuspid valves. ·
holosystolic
murmur ·
ejection type
murmur ·
third and
fourth heart sounds (gallop rhythm) ·
precordial lift ·
jugular venous
distention ·
pericardial
friction rub Key knowledge Cardiac
rhythm is classically described as regular, regularly irregular, or
irregularly irregular. Usually,
blood flows quietly through cardiac chambers and vessels. A heart “murmur” is caused by increased or
turbulent flow across a roughened surface, through a small hole, a narrowing,
or a damaged valve that is too tight (stenotic) or is leaking (regurgitant). Key knowledge The
first heart sound (called S1) is generated by closure of the
mitral and tricuspid valves, and has two components (M1 and T1). If
the aortic valve is stiff (or if there is severe hypertension) the aortic valve
may create an “ejection click” which will closely follow S1. The
second heart sound (S2) is generated by closure of the aortic and
pulmonic valves. It also has two
components (A2 and P2), that “split” into two closely
separated sounds during inspiration and merge into a single sound during
expiration?
Reference:
Richard J. McCarty, MD, Snap, Clickle, Plop, presentation notes, spring 2008. |
September 23
and 25, 2008
|
Note: Mental status exam was covered in Session 1. Hearing acuity, visual acuity, and
elevation of the palate were checked in Session 2. Cranial
Nerves: ____ CN I: test sense of smell. (Not usually done). Ask patient if there
has been any change in smell or taste. ____ CN II: (Note: visual acuity checked in Session
2) ____ CN III, IV, VI (oculomotor): check extraocular
motions in six positions of gaze and pupil reflex ____ CN V: Corneal reflex (not routine) ____ Sensation to light touch forehead, cheeks, jaw ____ Clench teeth while palpating masseters,
temporalis ____ CN VII: wrinkle forehead; try to open eyelids
closed tight; puff out cheeks; smile baring teeth ____ CN VIII: (Note: hearing acuity, Weber, and
Rinne tests were checked during Session 2). ____ CN IX (also CN X): On vocalizing “ah”, check for symmetric
elevation of palate. ____ CN IX: the gag reflex not routinely checked ____ CN X: Tested with CN IX above. Also, check quality of voice for dysphonia,
dysarthria. Ask about difficulty with
swallowing. ____ CN XI: Patient’s turns head left and right
against resistance. ____ Shoulder shrug against resistance. ____ CN XII: observe tongue for fasciculation. Have patient stick out tongue; check for
deviation. Neurologic
Examination Motor ____ Upper extremities: grip, biceps, triceps,
deltoid. ____ Lower extremities; iliopsoas, quadriceps,
hamstrings, foot dorsiflexion and plantar flexion. ____ With patient’s eyes closed, check for pronator
drift of the outstretched arms. ____ Test for increased muscle tone in the arms.
With the patient relaxed, move the elbow and wrist on each side, checking for
resistance, stiffness, tremor, cogwheeling. Cerebellar
____ Tap fingers repeatedly against the thumb, or
clap hands alternating one hand front-and-back to test rapid alternating
movements. ____ Have patient alternatively touch the tip of
their nose, then your fingertip as you move your hand. ____ Have patient touch their heel to the knee of
the opposite leg and slide it down the shin to the ankle. ____ Have the patient stand with feet together and
then close the eyes (Romberg test).
Watch for 20 sec. Sensory ____ Test light touch with monofilament on both feet
____ Test position sense on one digit on all four
limbs ____ Test vibration sense on both ankles or toes Reflexes ____ Cradle the arm across your forearm and test the
biceps, triceps, and brachioradialis reflexes. ____ With the patient’s legs dangling and hands
clenched together, test the patellar reflex. ____ Gently dorsiflex the foot and test Achilles
reflexes. ____ Stroke the sole of the foot in an arc to test
the plantar response. Documentation skills: on paper document your findings from the neurologic
exam. ____ cranial nerves ____ motor ____ cerebellar findings ____ sensory ____
reflexes |
Key Knowledge: The names and basic
function of the 12 cranial nerves. ·
I (olfactory):
sense of smell ·
II (optic):
visual image to brain ·
III
(oculomotor): Innervates levator palpebrae, superior,
medial,
inferior
rectus, inferior oblique, as well as the iris;
collectively these perform most eye movements. ·
IV
(trochlear): Innervates the superior oblique, which depresses and inward
rotates the eye. ·
V (trigeminal)
sensation from the face; motor to muscles of mastication ·
VI (abducens):
Innervates the lateral rectus, which abducts the eye (away
from nose). ·
VII (facial) motor
to the muscles of facial expression
and stapedius;
taste from the anterior 2/3 of the tongue; secretomotor
to the salivary glands (except parotid) and the lacrimal
gland, ·
VIII (vestibulocochlear) sound, rotation and gravity ·
IX (glossopharyngeal) taste from the posterior 1/3 of the tongue;
secretomotor to the parotid gland; motor to the stylopharyngeus
·
X (vagus)
branchiomotor to most laryngeal and pharyngeal muscles; parasympathetic
fibers to nearly all thoracic and abdominal viscera down to the splenic
flexure; receives taste from the epiglottis; motor to muscles of
voice and the soft palate. ·
XI (accessory)
muscles of the neck; overlaps with functions of the vagus. ·
XII (hypoglossal) motor to the muscles of the
tongue and other glossal muscles. Vocabulary ·
Upper and lower
motor neuron ·
Proprioception ·
Muscle tone ·
Clonus ·
Ataxia |
HPI:
![]() O = Onset: When did it begin
O = Onset: When did it begin
![]() P = Position, Pattern: one-sided, bend-like
P = Position, Pattern: one-sided, bend-like
![]() Q = Quality: sharp, dull, heavy, throbbing
Q = Quality: sharp, dull, heavy, throbbing
![]() R = Radiation (if pain)
R = Radiation (if pain)
![]() S = Severity: 1-10
S = Severity: 1-10
![]() T = Timing: with what activities does it occur
T = Timing: with what activities does it occur
![]() A = Aggravating/Alleviating: what makes it
better/worse?
A = Aggravating/Alleviating: what makes it
better/worse?
Have you
tried any medication?
![]() D =
Duration
D =
Duration
![]() A = Associated Symptoms
A = Associated Symptoms
a. Migraine:
i.
![]() Is there an aura?
Is there an aura?
ii.
![]() Are there scotomata or sensory/motor symptoms?
Are there scotomata or sensory/motor symptoms?
iii.
![]() Photophobia, phonophobia
Photophobia, phonophobia
b. ![]() Temporal
Arteritis:
Temporal
Arteritis:
i.
![]() Visual loss/eye
pain/diploplia
Visual loss/eye
pain/diploplia
ii.
![]() Proximal muscle
pain, jaw claudication
Proximal muscle
pain, jaw claudication
c. Brain tumor:
i.
![]() Weakness/dysequilibrium/neurologic
symptoms
Weakness/dysequilibrium/neurologic
symptoms
ii.
![]() Confusion or
lethargy
Confusion or
lethargy
iii.
![]() New onset
seizure
New onset
seizure
iv.
![]() New onset after
age 50
New onset after
age 50
v.
![]() Nocturnal
awakenings due to pain
Nocturnal
awakenings due to pain
vi.
![]() Worse with
valsalva
Worse with
valsalva
vii.
![]() Nausea/vomiting
Nausea/vomiting
viii.
![]() History of
malignancy
History of
malignancy
d. Meningitis:
i.
![]() Fever
Fever
ii.
![]() Neck
pain/stiffness
Neck
pain/stiffness
e. Subarachnoid
hemorrhage:
i.
![]() Family history
of migraine headache or subarachnoid hemorrhage
Family history
of migraine headache or subarachnoid hemorrhage
ii.
![]() Thunderclap
headache/onset with exertion
Thunderclap
headache/onset with exertion
f.
Cluster
headache:
i.
![]() Runny nose/nasal
congestion; lacrimation
Runny nose/nasal
congestion; lacrimation
ii.
![]() Headache around
the eye
Headache around
the eye
![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History
Medications:
![]() Use of headache medications: NSAID, Acetaminophen, prescription pain medications
or prescription migraine medications
Use of headache medications: NSAID, Acetaminophen, prescription pain medications
or prescription migraine medications
![]() Social
History:
Social
History:
![]() High Risk
Behaviors/Habits:
High Risk
Behaviors/Habits:
Family History:
![]() Family history of migraine headaches?
Family history of migraine headaches?
Physical Examination:
1. ![]() Vital signs (note or perform)
Vital signs (note or perform)
2. ![]() Cranial nerve exam
Cranial nerve exam
a. ![]() CN II (visual acuity, visual fields,
funduscopic exam)
CN II (visual acuity, visual fields,
funduscopic exam)
b. ![]() CN III, IV, VI (extraocular movements,
papillary light reflex [II/III])
CN III, IV, VI (extraocular movements,
papillary light reflex [II/III])
c. ![]() CN V (sensation of face, chewing
movements)
CN V (sensation of face, chewing
movements)
d. ![]() CN VII (facial expression)
CN VII (facial expression)
e. ![]() CN VIII (hearing)
CN VIII (hearing)
f. ![]() CN IX/X (symmetric elevation of soft
palate)
CN IX/X (symmetric elevation of soft
palate)
g. ![]() CN XI (head, neck, shoulder movements)
CN XI (head, neck, shoulder movements)
h. ![]() CN XII (tongue movements)
CN XII (tongue movements)
3. ![]() Palpate temporal arteries (particularly
if age > 50)
Palpate temporal arteries (particularly
if age > 50)
4. ![]() Screening motor examination
Screening motor examination
5. ![]() Palpate neck and shoulder muscles
Palpate neck and shoulder muscles
6. ![]() Screening sensory examination
Screening sensory examination
7. ![]() Reflexes
Reflexes
8. ![]() Cerebellar examination
Cerebellar examination
9. ![]() Gait
Gait
HPI:
1. ![]() O = Onset: When did it begin?
O = Onset: When did it begin?
2. ![]() P = Position, Pattern: unilateral, bilateral? upper
or lower extremities?
P = Position, Pattern: unilateral, bilateral? upper
or lower extremities?
3. ![]() Q =
Quality: Diffuse or focal?
Q =
Quality: Diffuse or focal?
4. ![]() R =
Radiation (if pain) (N/A)
R =
Radiation (if pain) (N/A)
5. ![]() S =
Severity: 1-10. compare to other weaknesses.
S =
Severity: 1-10. compare to other weaknesses.
6. ![]() T =
Timing: with what activities does it occur
T =
Timing: with what activities does it occur
7. ![]() A =
Aggravating/Alleviating
A =
Aggravating/Alleviating
a. ![]() Does
your weakness get worse with exercise? (Myasthenia
gravis)
Does
your weakness get worse with exercise? (Myasthenia
gravis)
8. ![]() D =
Duration
D =
Duration
9. ![]() A =
Associated Symptoms
A =
Associated Symptoms
a. ![]() Is it
difficult to participate in all activities? (often
due to functional weakness)
Is it
difficult to participate in all activities? (often
due to functional weakness)
b. ![]() Are
there any pains that affect or contribute to your weakness (think of diseases that cause muscle or joint pain – arthritis)
Are
there any pains that affect or contribute to your weakness (think of diseases that cause muscle or joint pain – arthritis)
c. ![]() Do you
have any numbness or tingling associated with your weakness? (MS, CVA, polyneuropathies)
Do you
have any numbness or tingling associated with your weakness? (MS, CVA, polyneuropathies)
d. ![]() Can you
see your muscles twitching? (ALS)
Can you
see your muscles twitching? (ALS)
e. ![]() Is the
weakness confined to 1 side of body (stroke,
TIA)
Is the
weakness confined to 1 side of body (stroke,
TIA)
 Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History
Associated with mononeuritis, polyneuropathies, and ischemic
stroke:
1.
![]() Diabetes
Diabetes
Associated with ischemic stroke:
1.
![]() Diabetes
Diabetes
2.
![]() Hypertension
Hypertension
3.
![]() Hypercholesterolemia
Hypercholesterolemia
4.
![]() History of
cigarette smoking
History of
cigarette smoking
Medications:
![]() Social
History:
Social
History:
![]() High Risk
Behaviors/Habits:
High Risk
Behaviors/Habits:
![]() Do you use tobacco?
Do you use tobacco?
![]() Family
History:
Family
History:
a.
![]() Any family
history of stroke or neurologic disease?
Any family
history of stroke or neurologic disease?
b.
![]() Any family history of hypertension?
Any family history of hypertension?
Physical Examination:
1.
![]() Inspection of the
muscle
Inspection of the
muscle
a.
![]() Atrophy
Atrophy
b.
![]() Enlargement
Enlargement
c.
![]() Fasciculations
Fasciculations
d.
![]() Ptosis
Ptosis
2.
![]() Palpation
Palpation
a.
![]() Muscle
tenderness
Muscle
tenderness
b.
![]() Increased tone
or rigidity
Increased tone
or rigidity
3.
![]() Motor exam
(muscle strength testing) using scale of 0-5.
Motor exam
(muscle strength testing) using scale of 0-5.
4.
![]() Ascertain
distribution of weakness
Ascertain
distribution of weakness
5.
![]() Assessment of
motor function (e.g., timed 50 foot walk)
Assessment of
motor function (e.g., timed 50 foot walk)
 Deep tendon reflexes
Deep tendon reflexes
HPI:
1. ![]() O = Onset: did the tremor start gradually or
abruptly?
O = Onset: did the tremor start gradually or
abruptly?
2. ![]() P = Position, Pattern: which parts of the body
are affected by the tremor?
P = Position, Pattern: which parts of the body
are affected by the tremor?
3. ![]() Q =
Quality:
Q =
Quality:
a.
![]() Does the tremor
occur at rest (Parkinson’s)
Does the tremor
occur at rest (Parkinson’s)
b.
![]() Does the tremor
occur with action (Action tremor,
essential tremor, cerebellar pathology, toxins)
Does the tremor
occur with action (Action tremor,
essential tremor, cerebellar pathology, toxins)
c.
![]() Does the tremor
interfere with daily activities
Does the tremor
interfere with daily activities
4. ![]() R =
Radiation (if pain)
R =
Radiation (if pain)
5. ![]() S =
Severity (1-10)
S =
Severity (1-10)
6. ![]() T =
Timing (with what activities does it occur)
T =
Timing (with what activities does it occur)
7. ![]() A =
Aggravating/Alleviating: Does stress, anxiety or fatigue increase or decrease
the tremor? (can occur with all tremor
types)
A =
Aggravating/Alleviating: Does stress, anxiety or fatigue increase or decrease
the tremor? (can occur with all tremor
types)
a. ![]() Does alcohol decrease the tremor?
Does alcohol decrease the tremor?
b. ![]() Does alcohol improve the tremor (65-70% of patients with essential tremor
report improvement with alcohol)?
Does alcohol improve the tremor (65-70% of patients with essential tremor
report improvement with alcohol)?
8. ![]() D =
Duration
D =
Duration
9. ![]() A =
Associated Symptoms
A =
Associated Symptoms
a.
![]() Gait disturbance
or falls (Parkinson’s, or secondary to
neuroleptic medication)
Gait disturbance
or falls (Parkinson’s, or secondary to
neuroleptic medication)
b.
![]() Neurologic
symptoms (muscle weakness, etc.)
Neurologic
symptoms (muscle weakness, etc.)
- Hyperthyroid symptoms (heat intolerance, weight
loss, etc.)
- Previous evaluation and treatment.
Allergies:
Past Medical & Past Surgical History
Medications:
a.
![]() Prescription
drugs: (theophylline, albuterol, valproic
acid, can
Prescription
drugs: (theophylline, albuterol, valproic
acid, can
cause postural
tremors)
![]() Social
History:
Social
History:
High Risk Behaviors/Habits:
1. ![]() Alcohol
Use
Alcohol
Use
a. ![]() Alcohol,
caffeine and nicotine, amphetamines (may
have an adrenergic enhancing effect).
Alcohol,
caffeine and nicotine, amphetamines (may
have an adrenergic enhancing effect).
![]() Family
History: is there a family history of
tremor?
Family
History: is there a family history of
tremor?
Physical Examination:
1.
![]() Thyroid Exam
Thyroid Exam
2. ![]() Observation of the tremor
Observation of the tremor
a. ![]() At rest
At rest
b. ![]() With action
With action
c. ![]() With standing
With standing
![]() 3. Observation of gait and stability
3. Observation of gait and stability
![]() 4. Motor exam
4. Motor exam
a. ![]() Check for increased muscle tone
(rigidity)
Check for increased muscle tone
(rigidity)
b. ![]() Check for slowed movements
(bradykinesia)
Check for slowed movements
(bradykinesia)
c. ![]() Muscle strength
Muscle strength
![]() 5. Coordination testing
5. Coordination testing
a. ![]() Finger tapping
Finger tapping
b. ![]() Rapid alternating movements
Rapid alternating movements
c. ![]() Finger-to-nose testing
Finger-to-nose testing
![]() 6. Mini-Cog
6. Mini-Cog
HPI:
Age of patient
ð O = Onset
ð P = Position, Pattern
ð Q= Quality
ð R= Radiation
ð S= Severity (1-10)
ð T= Timing (with what activities does it
occur)
ð A= Aggravating/Alleviating (including
medications)
ð D= Duration
ð A= Associated Symptoms
a.
Fevers/Chills
b.
Dysuria
c. Abdominal pain
d.
Unintentional weight loss
e.
Weakness/numbness
f. Fecal or urinary (overflow) incontinence
g. Gait disturbance
h. Pain
at rest
i. Nocturnal symptoms
a. Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History:
ð
1. History of malignancy
ð
2. Osteoporosis
ð
3. Recent intravenous catheter
ð
4. Immuocompromised state (chemotherapy, HIV, etc.)
Medications:
ð
1. Current or past steroid use
Social History:
High Risk Behaviors/Habits:
ð
1. Current or past IVDA
Family History:
Physical Examination:
ð
1. Vital signs
ð
2. Musculoskeletal
ð
a. Evaluation of movement and gait
ð
b. Inspection of spine and posture
ð
c. Palpation of spine and paraspinal muscles
ð
d. Straight leg raise test
ð
3. Neurologic exam
ð
a. Quadriceps strength (knee extension) – L3
ð
b. Dorsiflexion of ankle and great toe and/or
heel walk – L4/L5
ð
c. Ankle/foot plantarflexion or toe walk (S1)
ð
d. Light touch sensation
ð i. Anterior/lateral thigh – L3
ð ii. Medial ankle/foot – L4
ð iii. Dorsum of foot – L5
ð iv. Lateral plantar foot – S1
ð
e. Patellar reflex – L3/L4
ð
f. Achilles reflex – S1
□ How the symptoms started (open-ended)
□ a. Mechanism of injury or
trauma, if any
□ O= When symptoms started and duration of
pain
□ P=
Location of pain and radiation, if any
□ Q= Description/quality of pain
□ S= Severity of pain
□ T= Timing and frequency of the pain
□ A= Changes in pain since onset (worse,
less, etc)
a.
Aggravating/alleviating factors (including medications)
□ A=
Associated Symptoms
□ a. Tell how you use your
arms (or hands) at work or at home
□ b. Associated/alarm symptoms or
history
□ c. If arm complaint – is it
associated with chest pain or shortness of
breath
□ d. Numbness, burning or tingling
□ e. Neck complaints
□ f.
Redness
□
g. Swelling
□ h. Previous symptoms or
evaluation and treatment
Allergies:
Past Medical & Past Surgical History:
Medications:
Social History:
High Risk Behavior/Habits:
Family History:
PHYSICAL - Did the student correctly perform the
following physical exam skills (elbow, wrist OR hand):
Elbow
□
1.
Palpate lateral and medial
epicondyles
□ 2. Palpate
olecranon bursa and fossa
□ 3. Range
of Motion: Flexion
□ 4. Range
of Motion: Extension
□ 5. Range
of Motion: Supination
□ 6. Range
of Motion: Pronation
Wrist
□ 1. Palpate
soft tissue and carpals
□ 2. Palpate
ulnar styloid
□ 3. Range
of Motion: Flexion
□ 4. Range
of Motion: Extension
□ 5. Range
of Motion: Ulnar – Radial
□ 6. Perform
tests for Tinel’s Sign and Phalen’s Sign
Hand
□ 1. Palpate
C-MC joint of the thumbs
□ 2.
Palpate MCP joints of all digits
□ 3. Palpate
IP joints of the thumbs
□ 4. Palpate
PIP joints of all fingers
□ 5. Palpate DIP joints of all fingers
□ 6. Palpate
palmar fascia and tendons
□ 7. Range
of Motion: Making fist
□ 8. Range
of Motion: Making a claw by flexing
the
PIP and DIP joints
□ 9. Range
of Motion: Extension
□ 10. Check
grip strength
(optionally
with a sphygmomanometer)
HPI
Patient’s Name:
Age:
Occupation:
|
□ O = Onset □ P = Position, Pattern □ Q = Quality □ R = Radiation □ S = Severity (1-10) □ T = Timing (with what activities does it
occur) □ A = Aggravating/Alleviating (including
medications) □ D = Duration □ A = Associated symptoms? □ a. neck pain □ b. numbness/ tingling in arms. |
|
Allergies: |
|
Past Medical & Past Surgical History: □ 1. Previous shoulder injury □ 2. Ongoing medical conditions Medications: Social History: □ 1. Sports participation |
|
Family History: |
|
PHYSICAL EXAM – Did the student correctly perform the
following physical exam skills? |
|
□ 1. Look; expose both shoulders and
examine the skin, shape of the shoulders and posture of the arms? □ 2. Feel; for tenderness of the AC joint,
biceps tendon, and beneath the acromion
process? □ 3. Move the shoulder? a.
Assess active
ROM b.
Then assess
passive ROM □ 4. Perform
provocative testing □
a. AC joint □
b. Subacromion space □
c. Supraspinatus □ d. Infraspinatus & teres minor □
e. Subscapularis □
f. Biceps □ g. Glenohumeral joint □ h.
Cervical nerve root |
HPI:
Age of patient
![]() O = Onset
O = Onset
![]() P = Position, Pattern, Location
P = Position, Pattern, Location
![]() Q = Quality (type of pain)
Q = Quality (type of pain)
![]() a. Pressure, aching, tearing, sharp, pleuritic, etc.
a. Pressure, aching, tearing, sharp, pleuritic, etc.
![]() R = Radiation
R = Radiation
![]() a. Jaw, neck
a. Jaw, neck
![]() b. Left and/or right arms
b. Left and/or right arms
![]() c. Back
c. Back
![]() d. Epigastrum
d. Epigastrum
![]() S = Severity (1-10)
S = Severity (1-10)
![]() T = Timing (with what activities does it occur)
T = Timing (with what activities does it occur)
![]() A = Aggravating
A = Aggravating
![]() a. Exercise
a. Exercise
![]() b. Stress
b. Stress
![]() c. Eating
c. Eating
![]() d. Laying
down
d. Laying
down
![]() Alleviating
Alleviating
![]() e. Rest
e. Rest
![]() f.
Nitroglycerin
f.
Nitroglycerin
![]() g. Sitting
up/leaning forward
g. Sitting
up/leaning forward
![]() h. Antacids
h. Antacids
![]() D = Duration
D = Duration
![]() A = Associated Symptoms
A = Associated Symptoms
![]() a. Nausea/vomiting
a. Nausea/vomiting
![]() b. Diaphoresis
b. Diaphoresis
![]() c. Syncope or pre-syncope
c. Syncope or pre-syncope
![]() d. Dyspnea
d. Dyspnea
![]() e. Hemoptysis
e. Hemoptysis
![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History
 Coronary Heart Disease
Coronary Heart Disease Diabetes Mellitus
Diabetes Mellitus- Hypertension
 Dyslipidemia
Dyslipidemia- Peripheral arterial disease
- Chronic Kidney Disease
Medications:
- General
Social History:
High Risk Behaviors/Habits:
- Tobacco
 Cocaine
Cocaine
Family History:
- Premature CHD
 Venous thromboembolism
Venous thromboembolism
Physical Examination:
- General Appearance
- Vital signs and (if possible) Body Mass Index
- BP in both arms if aortic dissection is being
considered
- Cardiovascular examination
- Inspection of chest wall (including skin for
rashes)
- Palpation of chest wall (reproducibility of
chest pain) and PMI
- Auscultation
i.
![]() Sitting
Sitting
ii.
![]() Supine
Supine
iii.
![]() Left lateral decubitus (S3, S4, mitral stenosis)
Left lateral decubitus (S3, S4, mitral stenosis)
 Jugular venous pressure
Jugular venous pressure Pulmonary examination
Pulmonary examination- Auscultation: anterior, posterior, lateral
- Percussion: anterior, posterior, lateral
- Abdominal examination
- Auscultation
- Palpation, light and deep
- Palpation of the aorta
- Extremities
- Pulses
i.
![]() Radial (note symmetry)
Radial (note symmetry)
ii.
![]() Posterior tibial, dorsalis pedis
Posterior tibial, dorsalis pedis
- Assessment of edema
HPI:
Age of patient
![]() 1. O = Onset
1. O = Onset
![]() 2. P = Position, Pattern
2. P = Position, Pattern
a. ![]() Does the cough occur lying down?
Does the cough occur lying down?
3. ![]() Q = Quality
Q = Quality
a. ![]() Dry vs. productive
Dry vs. productive
4. ![]() R = Radiation N/A
R = Radiation N/A
5. ![]() S = Severity
S = Severity
6. ![]() T = Timing (with what activities does it occur)
T = Timing (with what activities does it occur)
7. ![]() A = Aggravating/Alleviating
A = Aggravating/Alleviating
8. ![]() D = Duration
D = Duration
9. ![]() A = Associated Symptoms
A = Associated Symptoms
a. ![]() Hemoptysis
Hemoptysis
b. ![]() Shortness of breath
Shortness of breath
c. ![]() Lower extremity edema
Lower extremity edema
d. ![]() Fever, chills
Fever, chills
e. ![]() Wheezing
Wheezing
f.![]() Rhinitis/post-nasal drip/nasal congestion
Rhinitis/post-nasal drip/nasal congestion
g. ![]() Recent upper respiratory tract infection
Recent upper respiratory tract infection
h. ![]() Heartburn/GERD symptoms
Heartburn/GERD symptoms
10. ![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History:
 Hypertension
Hypertension Coronary heart disease/CHF
Coronary heart disease/CHF Asthma/COPD
Asthma/COPD- Allergic rhinitis/seasonal allergies
- Previous pneumonia; if so, when
- GERD
- Sinusitis (recent, recurrent, chronic)
Medications:
 General
General Angiotensin-converting enzyme inhibitors
Angiotensin-converting enzyme inhibitors- Any medications added recently
Social History:
High Risk Behaviors/Habits:
- Tobacco
Family History:
Physical Examination:
![]() 1. General
appearance
1. General
appearance
- Vital signs
- HEENT examination
- Nasal passages for congestion, drainage
- Throat
- Ears (otoscope)
- Sinus palpation and transillumination (if
appropriate)
- Neck/adenopathy
- Pulmonary examination
- Inspection (anterior-posterior diameter)
- Auscultation: anterior, posterior, lateral
i.
![]() Forced expiration
Forced expiration
- Percussion: anterior, posterior, lateral
- Abdominal examination
- Auscultation
- Palpation: light, deep
HPI:
Age of patient
![]() 1. O = Onset
1. O = Onset
![]() 2. P = Position, Pattern
2. P = Position, Pattern
a. ![]() Dyspnea at rest
Dyspnea at rest
b. ![]() Dsypnea on exertion
Dsypnea on exertion
c. ![]() Orthopnea
Orthopnea
d. ![]() Paroxysmal nocturnal dyspnea
Paroxysmal nocturnal dyspnea
3. ![]() Q = Quality
Q = Quality
a. ![]() Hard to take a deep breath, increased effort to
breath, etc.
Hard to take a deep breath, increased effort to
breath, etc.
4. ![]() R = Radiation N/A
R = Radiation N/A
5. ![]() S = Severity
S = Severity
6. ![]() T = Timing (with what activities does it occur)
T = Timing (with what activities does it occur)
7. ![]() A = Aggravating
A = Aggravating
a. ![]() Exertion
Exertion
b. ![]() Laying flat
Laying flat
c. ![]() Anxiety
Anxiety
Alleviating
d. ![]() Rest
Rest
e. ![]() Sitting up
Sitting up
8. ![]() D = Duration, chronology
D = Duration, chronology
a. ![]() Progression of symptoms (improving, stable, worsening)
Progression of symptoms (improving, stable, worsening)
9. ![]() A = Associated Symptoms (as appropriate)
A = Associated Symptoms (as appropriate)
a. ![]() Cough
Cough
b. ![]() Hemoptysis
Hemoptysis
c. ![]() Fever, chills
Fever, chills
d. ![]() Lower extremity edema
Lower extremity edema
e. ![]() Chest pain/pressure
Chest pain/pressure
f.![]() Wheezing
Wheezing
g. ![]() Anxiety
Anxiety
h. ![]() Decreased urine output
Decreased urine output
10. ![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History:
- COPD/Asthma
- Coronary heart disease/congestive heart failure
- Valvular heart disease
- Venous Thromobembolism (DVT, PE)
- Collagen-Vascular disease
- Anemia
- Kidney disease
- Diabetes Mellitus
Medications:
- General
- Any medications started recently
Social History:
High Risk Behaviors/Habits:
- Tobacco use
Family History:
- Premature CHD
- Venous thromboembolism
Physical Examination:
- General appearance
- Able to speak full sentences
- Vital signs, including respiratory rate
- Pulmonary examination
- Inspection
i.
![]() Use of respiratory accessory muscles, work of
breathing
Use of respiratory accessory muscles, work of
breathing
ii.
![]() Check for increased anterior-posterior diameter
Check for increased anterior-posterior diameter
- Auscultation: anterior, posterior, lateral
- Percussion: anterior, posterior, lateral
- Expansion (symmetric)
- Cardiac examination
- Inspection
- Palpation of PMI
- Auscultation
i.
![]() Sitting
Sitting
ii.
![]() Supine
Supine
iii.
![]() Left lateral decubitus (S3, S4, mitral stenosis)
Left lateral decubitus (S3, S4, mitral stenosis)
- Jugular venous pressure
- Extremities
- Assessment of lower extremity edema
- Assessment for clubbing
- Assessment for cyanosis
HPI:
Age of patient
![]() 1. O= Onset
1. O= Onset
2. ![]() P = Position, Pattern, Location
P = Position, Pattern, Location
a. ![]() Unilateral vs. bilateral
Unilateral vs. bilateral
b. ![]() Peripheral vs. central or diffuse
Peripheral vs. central or diffuse
3. ![]() Q = Quality N/A
Q = Quality N/A
4. ![]() R = Radiation N/A
R = Radiation N/A
5. ![]() S = Severity
S = Severity
6. ![]() T = Timing (with what activities does it occur)
T = Timing (with what activities does it occur)
a. ![]() Intermittent vs. persistent
Intermittent vs. persistent
b. ![]() All day vs. present in the evening, etc.
All day vs. present in the evening, etc.
7. ![]() A = Aggravating/Alleviating
A = Aggravating/Alleviating
8. ![]() D = Duration
D = Duration
a. ![]() Progression
Progression
9. ![]() A = Associated Symptoms (in addition to those in other
categories)
A = Associated Symptoms (in addition to those in other
categories)
a. ![]() General (occurs with multiple etiologies):
General (occurs with multiple etiologies):
i.
![]() Weight gain; if so, time frame
Weight gain; if so, time frame
ii.
![]() Shortness of breath/dyspnea on exertion
Shortness of breath/dyspnea on exertion
b. ![]() Allergy and anaphylaxis
Allergy and anaphylaxis
i.
![]() Sensation of swelling in throat/lips
Sensation of swelling in throat/lips
c. ![]() Congestive heart failure
Congestive heart failure
i.
![]() Waking up at night short of breath (paroxysmal
nocturnal dyspnea)
Waking up at night short of breath (paroxysmal
nocturnal dyspnea)
ii.
![]() Sleeping with head raised up (orthopnea)
Sleeping with head raised up (orthopnea)
d. ![]() Venous thromboembolism
Venous thromboembolism
i.
![]() Unilateral leg edema/pain
Unilateral leg edema/pain
ii.
![]() Pleuritic chest pain
Pleuritic chest pain
iii.
![]() Hemoptysis
Hemoptysis
iv.
![]() Recent immobility
Recent immobility
e. ![]() Cirrhosis
Cirrhosis
i.
![]() Abdominal distension
Abdominal distension
ii.
![]() Jaundice (skin/eyes)
Jaundice (skin/eyes)
10. ![]() Previous
evaluation and treatment
Previous
evaluation and treatment
Allergies:
- Known allergies and any recent exposure to them
Past Medical & Past Surgical History
- Coronary Heart Disease and/or CHF
- Hypertension
- Valvular heart disease or Rheumatic Fever
- Kidney disease
- Diabetes Mellitus
- Liver disease, hepatitis B/C
- Venous thromboembolism (PE or DVT)
- Malignancy
- Recent surgery
Medications:
- General
- Calcium-channel blockers
- NSAIDs
- Angiotensin-coverting enzyme inhibitors or
angiotensin receptor blockers (especially recently prescribed)
Social History:
- Diet: sodium intake (restaurants, processed
foods)
High Risk Behaviors/Habits:
- Alcohol intake
- IVDA
Family History:
- Venous thromboembolism
- Premature CHD
Physical Examination:
![]() 1. General
appearance
1. General
appearance
![]() 2. Vital signs
2. Vital signs
- Cardiac examination
- Inspection
- Palpation of PMI
- Auscultation
i.
![]() Sitting
Sitting
ii.
![]() Supine
Supine
iii.
![]() Left lateral decubitus (S3, S4, mitral stenosis)
Left lateral decubitus (S3, S4, mitral stenosis)
iv.
![]() Jugular venous pressure
Jugular venous pressure
- Pulmonary examination
- Auscultation: anterior, posterior, lateral
- Percussion: anterior, posterior, lateral
- Abdominal examination
- Inspection: caput medusa, distension
- Auscultation
- Palpation, light and deep
i.
![]() Palpate liver edge using correct technique
Palpate liver edge using correct technique
ii.
![]() Check for splenomegaly
Check for splenomegaly
- Percussion
i.
![]() Liver span
Liver span
ii.
![]() Traube’s space
Traube’s space
- Extremities
- Check for edema
i.
![]() Check for pre-sacral edema
Check for pre-sacral edema
HPI:
Age of patient
1. ![]() O = Onset
O = Onset
2. ![]() P = Position, Pattern N/A
P = Position, Pattern N/A
3. ![]() Q = Quality/quantity
Q = Quality/quantity
a. ![]() Amount
Amount
b. ![]() Color
Color
c. ![]() Presence of sputum
Presence of sputum
4. ![]() R = Radiation N/A
R = Radiation N/A
5. ![]() S = Severity (relates to amount, above)
S = Severity (relates to amount, above)
6. ![]() T = Timing/frequency
T = Timing/frequency
7. ![]() A = Aggravating/Alleviating
A = Aggravating/Alleviating
8. ![]() D = Duration
D = Duration
9. ![]() A = Associated Symptoms
A = Associated Symptoms
a. ![]() Chest pain
Chest pain
b. ![]() Cough: acute or chronic
Cough: acute or chronic
c. ![]() Shortness of breath
Shortness of breath
d. ![]() Fevers, chills, night sweats
Fevers, chills, night sweats
e. ![]() Weight loss
Weight loss
f.![]() Recent immobility
Recent immobility
g. ![]() Nose bleeds or bleeding elsewhere
Nose bleeds or bleeding elsewhere
h. ![]() Sinus symptoms
Sinus symptoms
i. ![]() Nausea, vomiting
Nausea, vomiting
j. ![]() Dyspepsia
Dyspepsia
10. ![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History
- Recent surgery
 Venous thromboembolism (PE or DVT)
Venous thromboembolism (PE or DVT) Malignancy
Malignancy- Pulmonary disease/chronic cough
- Asthma or COPD
- Recurrent pneumonia
- TB, TB exposure, +PPD
- Sinusitis/allergic rhinitis
- Cardiac disease
- Valvular heart disease
- Congestive heart failure
- Thrombocytopenia or bleeding disorders
- Liver disease
- Peptic ulcer disease
![]() 10. HIV
10. HIV
![]() 11.
Collagen-vascular disease
11.
Collagen-vascular disease
Medications:
- General
- Warfarin
- Aspirin, NSAIDs
- Oral contraceptives
Social History:
1.
![]() Recent travel
Recent travel
a.
![]() Duration of plane ride
Duration of plane ride
b.
![]() Travel to areas endemic for TB
Travel to areas endemic for TB
2.
![]() Blood transfusions (especially before 1985)
Blood transfusions (especially before 1985)
High Risk Behaviors/Habits:
- Tobacco
- Cocaine
- Intravenous drug use
- High risk sexual practices
Family History:
- Venous thromboembolism
Physical Examination:
- General appearance
- Vital signs including respiratory rate
- Skin: inspection for bruising
- HEENT examination
- Inspection of nares
- Inspection of oropharynx
- Pulmonary examination
- Inspection
i.
![]() Work of breathing
Work of breathing
ii.
![]() (Respiratory rate if not taken with vitals)
(Respiratory rate if not taken with vitals)
- Auscultation: anterior, posterior, lateral
- Percussion: anterior, posterior, lateral
- Cardiovascular examination
- Inspection
- Auscultation
i.
![]() Sitting
Sitting
ii.
![]() Supine
Supine
iii.
![]() Left lateral decubitus (S3, S4, mitral stenosis)
Left lateral decubitus (S3, S4, mitral stenosis)
- Jugular venous pressure
- Abdominal examination
- Inspection
- Auscultation
- Palpation, light and deep
- Extremities
- Assessment of edema
HPI:
Age of patient
![]() O = Onset/Offset
O = Onset/Offset
a. ![]() Gradual vs. abrupt
Gradual vs. abrupt
![]() P = Position, Pattern
P = Position, Pattern
a. ![]() Positional component
Positional component
b. ![]() Regular vs. irregular
Regular vs. irregular
c. ![]() Tap out rhythm of the palpitations
Tap out rhythm of the palpitations
![]() Q = Quality
Q = Quality
d. ![]() Fluttering, racing, slow, pounding/flip-flopping, etc.
Fluttering, racing, slow, pounding/flip-flopping, etc.
![]() R = Radiation
R = Radiation
e. ![]() To neck
To neck
![]() S = Severity
S = Severity
![]() T = Timing (with what activities does it occur)
T = Timing (with what activities does it occur)
![]() A = Aggravating/Alleviating
A = Aggravating/Alleviating
f.![]() Are symtoms terminated by valsalva or rubbing neck?
Are symtoms terminated by valsalva or rubbing neck?
![]() D = Duration
D = Duration
![]() A = Associated Symptoms
A = Associated Symptoms
g. ![]() Anxiety
Anxiety
h. ![]() Alarm symptoms
Alarm symptoms
i.
![]() Syncope or pre-syncope
Syncope or pre-syncope
ii.
![]() Chest pain
Chest pain
iii.
![]() Shortness of breath
Shortness of breath
![]() Previous evaluation and treatment
Previous evaluation and treatment
Allergies:
Past Medical & Past Surgical History
- Cardiac disease: Coronary heart disease, CHF,
valvular heart disease
- Hypertension
- Thyroid disease
- Diabetes Mellitus
- Psychiatric illness
Medications:
- General
- Levothyroxine
- Beta-blockers recently stopped
Family History:
1. ![]() Student provides summary to patient
Student provides summary to patient
Social History/ High Risk Behaviors/Habits:
- Nicotine
- Cocaine
- Amphetamines
- Caffeine intake
Physical Examination:
- General appearance
- Vital signs
- Neck: examination of the thyroid
- Cardiac examination
- Inspection
- Palpation of PMI
- Auscultation
i.
![]() Sitting
Sitting
ii.
![]() Supine
Supine
iii.
![]() Left lateral decubitis (S3, S4, mitral stenosis)
Left lateral decubitis (S3, S4, mitral stenosis)
- Examination of Jugular veins
i.
![]() Pattern
Pattern
ii.
![]() Estimate jugular venous pressure
Estimate jugular venous pressure
- Pulmonary examination
- Auscultation, anterior and posterior
- Percussion, anterior and posterior
- Extremities
- Assessment of edema
- Pulses: posterior tibial, dorsalis pedis
- Student performed oral presentation to group